|
History
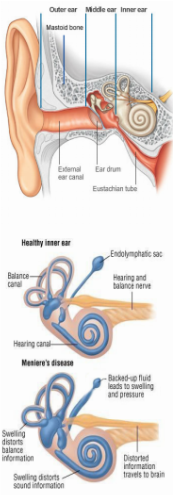
In 1861, a French doctor Prosper Menière, named a syndrome of “attacks” of extreme dizziness, abnormal ringing in the ears, temporary total loss of balance accompanied by nausea and vomiting or a combination of all symptoms. He recognised symptoms were an inner ear dysfunction, a novel idea at the time. Today, Meniere’s Disease or “MD” is still thought incurable. Theories of cause vary as much as treatments; vascular insuciency, virus, autoimmune, congenital, genetic, hormonal and others. Many studies document disability indices, quality of life, family heritability, involvement of one or both ears, association with stress, menstruation, diet, migraine variants, concurrent conditions, geographic spread and ethnic distribution. Conventional MD treatment often climbs a ladder as time progresses. With its waxing and waning condition and variability, treatment is mainly symptom management and if severe enough, eventual destructive surgery and cochlear implants. Many diagnosed are left with hearing loss and chronic imbalance. It is now known that the condition is cochleovestibular oedema where too much endolymphatic fluid swells the cochlea and vestibular spaces called endolymphatic hydrops. MD is ruled in when endolymphatic hydrops from syphilis, Paget’s, trauma, Lyme and others are ruled out. MD is therefore idiopathic (unknown cause) endolymphatic hydrops. How does Ménière’s disease affect you? Symptoms vary between people and over time. The main problems are unpredictable attacks of vertigo with nausea and vomiting. Attacks can last from a few minutes to 24 hours. There may also be tinnitus, hearing loss and a feeling of fullness in the affected ear. Periods of remission between attacks can vary from days to months or even years; making Ménière’s an unpredictable and distressing illness. As it progresses the vertigo may be less severe; however there may be periods of imbalance, adding to the distress. In the later stages tinnitus is more prominent and fluctuating hearing loss develops. There is permanent damage to the balance organ and significant balance problems are common. Usually only one ear is affected, but up to 50% of sufferers may develop the condition in both ears. It is useful to divide the course of the illness into three stages: Stage one (early): unpredictable attacks of vertigo The main feature is intermittent attacks of vertigo which can last from a few minutes to hours. During the attack there is a variable amount of hearing loss along with a sensation of fullness in the affected ear. Some people may experience tinnitus or an increase in tinnitus in the affected ear. The fullness in the ear and tinnitus may precede the attacks of vertigo, but they will often occur without warning. In between the attacks the hearing and sensation in the ear return to normal. There are periods of remission between the attack, which vary in each person making Ménière’s disease an unpredictable and distressing illness. Stage two (intermediate): attacks of vertigo; tinnitus; hearing loss The attacks of vertigo continue with variable remissions however may be less severe. After or perhaps before the attack the person may experience a period of imbalance and movement induced giddiness. Permanent hearing loss develops and continues to fluctuate with the vertigo attacks. Tinnitus becomes more prominent often fluctuating or increasing with the attacks. Stage three (late): hearing loss; balance difficulties; tinnitus In the later stages the hearing loss increases and often the attacks of vertigo diminish or stop. Hearing loss can be severe and distortion, loudness discomfort and recruitment can be a problem. There is permanent damage to the balance organ in the ear and significant general balance problems are common, especially in the dark |
|
